
When you’re on a combination of NTI drugs, even a tiny change in dosage can be dangerous. These aren’t ordinary medications. They’re the kind where the difference between healing and harm is razor-thin. Think warfarin, lithium, or levothyroxine - drugs that require constant monitoring because a small shift in blood levels can cause a stroke, seizure, or thyroid crisis. Now imagine taking two of them together in a single pill. That’s a combination NTI therapy. And here’s the problem: almost none of them have generic versions in the U.S., even though single-component generics are widely available.
What Makes NTI Drugs So Risky?
NTI stands for Narrow Therapeutic Index. That means the amount of drug needed to work is almost the same as the amount that can poison you. For most medications, your body can handle some variation - maybe you take a 5% higher dose by accident, and nothing happens. But with NTI drugs, that 5% could mean the difference between a stable INR and a life-threatening bleed. The FDA says these drugs have five key traits: minimal gap between effective and toxic levels, risk of serious side effects from small concentration changes, need for regular blood tests, low variation within the same person over time, and frequent small dose tweaks in real-world use.
Examples include warfarin (blood thinner), digoxin (heart medication), phenytoin (seizure control), and lithium (mood stabilizer). Each of these has multiple generic versions approved. But when you combine two NTI drugs - say, warfarin and amiodarone - you’re doubling the risk. A 10% fluctuation in one drug might be manageable. A 10% fluctuation in two? That’s a 20% total variation in your system. And that’s exactly what happens when you switch from brand-name to generic in a fixed-dose combo.
Why Don’t Generic Combination NTI Drugs Exist?
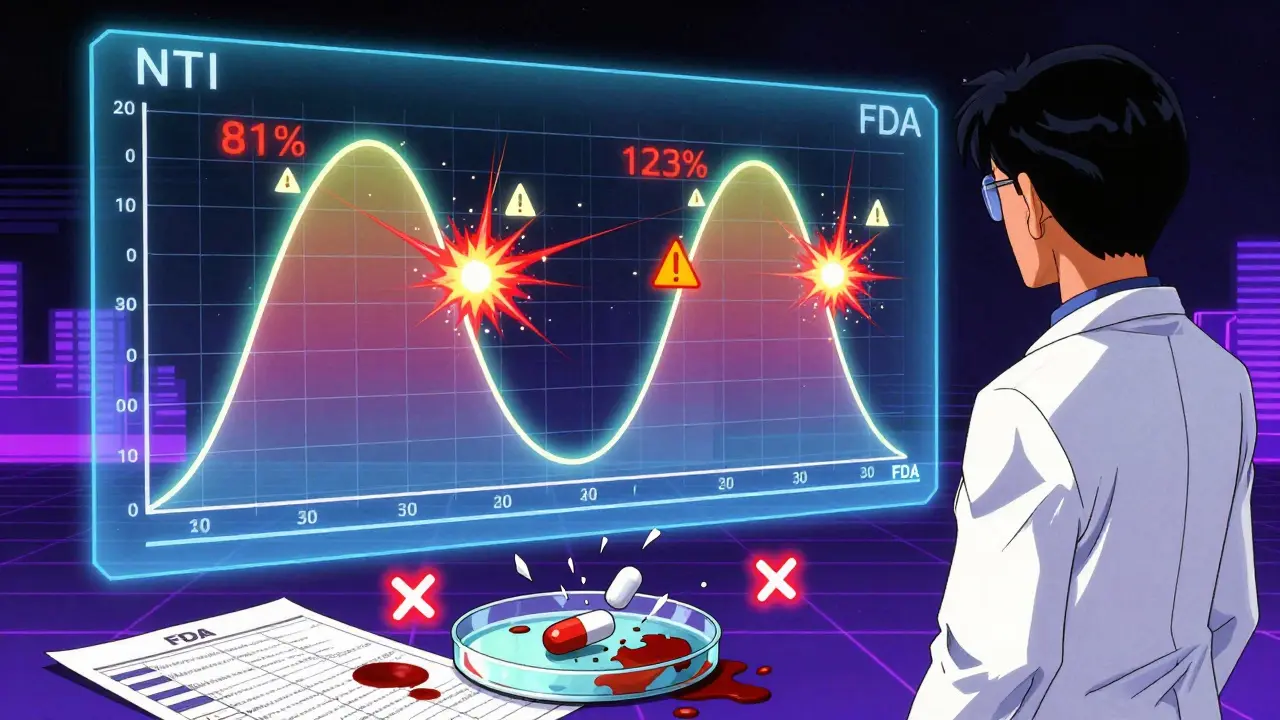
The FDA set strict bioequivalence rules for NTI drugs back in 2014, then tightened them again in 2022. For regular drugs, generics must match the brand within 80%-125% of the original for absorption (AUC) and peak levels (Cmax). For NTI drugs, that window shrinks to 90%-111% for Cmax and 90%-112% for AUC. That’s already a huge hurdle. But when you have a pill with two NTI drugs inside? The math gets impossible.
Let’s say Drug A has a 90%-111% bioequivalence range. Drug B does too. When combined, the total variation isn’t 90%-111% - it’s 90% of 90% to 111% of 111%. That’s 81%-123%. That’s wider than the standard range for non-NTI drugs. The FDA’s own 2023 draft guidance now proposes even tighter limits for multi-NTI combinations: 90%-107.69% for Cmax and 90%-110% for AUC. No manufacturer has yet figured out how to consistently hit those numbers in a fixed-dose pill. So, no approvals.
Compare that to non-NTI combos like entecavir/tenofovir for HIV - dozens of generics exist. But for NTI combos? The FDA Orange Book shows only 12.6% of combination regimens involving NTI drugs have any generic version. For warfarin alone, there are 11 approved generics. For warfarin plus another NTI? Zero.
What Happens When Patients Get Switched Anyway?
Even though fixed-dose NTI combos aren’t approved as generics, patients still get switched - often by accident. Pharmacies substitute single NTI drugs in a regimen. A patient on brand-name warfarin and brand-name amiodarone might get generic warfarin. Or worse, both get switched at once. The consequences aren’t theoretical.
A 2020 JAMA Internal Medicine study found that when patients on a combination containing one NTI drug were switched to generics, they had a 27% higher chance of adverse events compared to 8% for non-NTI combos. A Drugs.com survey of 1,247 patients on NTI combinations showed 63.4% reported problems after generic substitution - things like erratic INR levels, tremors, or hospitalizations. One patient on Reddit described his INR jumping from 2.5 to 6.8 after a pharmacy switch - a level that caused internal bleeding. He was hospitalized. His doctors said it was avoidable.
Pharmacists are seeing it too. A 2023 ASHP survey of 856 pharmacists found 78.3% had witnessed therapeutic failure after generic substitution in NTI-containing regimens. Over 40% reported serious adverse events. That’s not a glitch. That’s a systemic risk.
Who’s Against Generic NTI Combos - And Why?
The American Society of Health-System Pharmacists (ASHP) says automatic substitution of NTI drugs in combination therapy is “unacceptable.” They’re not alone. Dr. Aaron Kesselheim from Harvard showed in a 2015 JAMA study that 18.7% of patients on generic warfarin had unstable INR levels - compared to just 4.3% on brand. When you combine that with another NTI drug, the numbers get worse. Dr. Janet Woodcock, former head of FDA’s drug center, said plainly: “NTI drugs require special consideration. Combination products present even greater scientific challenges.”
Some experts argue the problem isn’t the drugs - it’s the standards. Dr. Donald Berry, in Nature Reviews Drug Discovery, pointed out that even the tightened 90%-111% window still allows 22% total variation. When two drugs are combined, that variation multiplies. “We’re asking manufacturers to hit a target that doesn’t exist in real-world physiology,” he said.
But it’s not all doom. In Europe, generic levothyroxine combinations have been used since 2015 with less than 2% adverse event rates. The EMA uses similar standards to the FDA but has approved a few combo products. Why the difference? Some believe it’s because European systems rely more on pharmacist-led monitoring and tighter tracking of patient outcomes. The U.S. system doesn’t have that infrastructure in place.
The Real Cost of Not Having Generics
Patients on combination NTI therapy pay more - and pay more in other ways too. Annual therapeutic drug monitoring costs $1,200-$2,500 per patient, compared to $400-$800 for non-NTI combos. That’s because you need frequent blood tests to catch tiny shifts. Stabilizing a patient on a combo NTI regimen takes 6-8 weeks and an average of 3.2 dose adjustments. For non-NTI combos? Just 1.8 adjustments.
And the burden isn’t just financial. Clinicians need specialized training - 120+ hours, according to ASHP - to manage these regimens. Most community pharmacies don’t have that expertise. Only 12 of 50 major U.S. academic medical centers have dedicated NTI combination therapy clinics. That means most patients are managed by providers who’ve never been trained to handle this complexity.
Documentation is worse too. FDA-approved NTI monotherapy labels average 4.2 out of 5 for clarity. Combination NTI labels? 2.8 out of 5. That’s not just inconvenient - it’s dangerous.
What’s Next? Will Generics Ever Come?
The FDA is working on a pilot program for 2024 called “precision bioequivalence,” using pharmacometric modeling to predict how combinations behave in real patients. That’s a step forward. But experts are divided. Dr. Robert Temple, a former FDA official, thinks better manufacturing will eventually make it possible. Dr. Lewis Nelson from NYU disagrees. “The fundamental pharmacokinetic challenges,” he says, “make true therapeutic equivalence unattainable with current technology.”
Right now, the market for NTI drugs is worth nearly $49 billion globally. But combination NTI products? Less than 0.3% of that. The science, the regulation, the monitoring - it’s all stacked against them. Until we have better tools to measure real-time drug interaction in individuals - not just averages in clinical trials - combination NTI generics will remain a gap.
Until then, patients and providers are stuck. They’re forced to choose between expensive brand-name combos or risking instability by switching single components. Neither option is ideal. And for people who need both drugs to survive - like those with complex arrhythmias or treatment-resistant epilepsy - the gap isn’t just a policy issue. It’s a matter of life and death.
What Can Patients Do?
- Ask your pharmacist: “Is this medication part of an NTI combo? Are both drugs brand or generic?”
- If you’re on a combination with any NTI drug, never let your pharmacy switch one without telling you.
- Request a prescription that says “Do Not Substitute” if your regimen includes NTI drugs.
- Keep a log of your symptoms and lab results - even small changes matter.
- Ask your doctor if you qualify for a specialty clinic that monitors NTI combos.
There’s no easy fix. But awareness can prevent harm. The system isn’t designed for these drugs. Patients have to be their own advocates.
What are NTI drugs?
NTI stands for Narrow Therapeutic Index. These are medications where the difference between an effective dose and a toxic dose is very small. Examples include warfarin, lithium, levothyroxine, phenytoin, and digoxin. Even small changes in blood levels can lead to serious side effects or treatment failure. They require careful dosing and frequent monitoring.
Why are generic combination NTI drugs not available in the U.S.?
Combining two NTI drugs in one pill creates an almost impossible bioequivalence challenge. The FDA requires extremely tight limits on how much a generic can vary from the brand - 90%-111% for peak levels and 90%-112% for total absorption. When two such drugs are combined, the total variation multiplies, making it nearly impossible to meet the standard. No manufacturer has yet proven their product meets the FDA’s 2023 draft guidelines for multi-NTI combinations.
Can I switch from brand to generic if I’m on a combination NTI therapy?
It’s risky. Even switching one drug in a combination that includes an NTI drug can cause instability. Studies show a 27% higher rate of adverse events when generics are substituted in NTI-containing regimens. Always ask your doctor and pharmacist before any switch. Request a "Do Not Substitute" prescription if you’re on an NTI combo.
How do I know if my medication is an NTI drug?
Check the FDA’s list of NTI drugs, available through the Orange Book. Common ones include warfarin, levothyroxine, lithium, phenytoin, digoxin, and carbamazepine. Your pharmacist can also tell you. If your drug requires frequent blood tests (like INR for warfarin or TSH for thyroid meds), it’s likely an NTI drug.
Are there any safe generic combination NTI drugs anywhere?
A few have been approved in Europe, such as generic levothyroxine combinations, with less than 2% adverse event rates. These use strict monitoring and pharmacist-led protocols. In the U.S., no fixed-dose combination of two NTI drugs has been approved. Some patients report success with separate generic NTI drugs under close supervision, but that’s not the same as a fixed-dose combo.
What’s being done to fix this gap?
The FDA is testing a new method called "precision bioequivalence" using computer modeling to predict how combination NTI drugs behave in real patients. This pilot program starts in 2024. It could lead to new approval standards that better reflect clinical reality. But experts warn that until we can measure individual drug interactions accurately, true equivalence will remain out of reach.







Comments
Gregory Parschauer
January 13, 2026This is why America’s healthcare system is a goddamn circus. You’ve got patients on life-saving meds, and the FDA’s playing Tetris with bioequivalence thresholds like it’s a spreadsheet exercise. 90%-111%? That’s not science - that’s corporate laziness dressed up as regulation. I’ve seen INR levels swing like a pendulum after a pharmacy switch, and no, it’s not ‘user error.’ It’s systemic negligence. And don’t even get me started on how pharmacies auto-substitute without telling anyone. This isn’t about cost - it’s about control. Someone’s making bank off brand-name combos while patients bleed out in waiting rooms.
Acacia Hendrix
January 14, 2026Let’s be clear: the bioequivalence paradigm for multi-NTI combinations is fundamentally flawed because it assumes pharmacokinetic additivity - a gross oversimplification of nonlinear drug interactions. The FDA’s 2023 draft guidance, while well-intentioned, fails to account for inter-individual variability in CYP450 metabolism, plasma protein binding, and transporter polymorphisms. Until we move beyond population-based AUC/Cmax metrics and adopt individualized pharmacometric modeling - which, frankly, is still in its infancy - any claim of ‘therapeutic equivalence’ is pseudoscientific theater. This isn’t a regulatory gap. It’s a conceptual one.
vishnu priyanka
January 15, 2026Man, I read this and thought about my uncle back in Kerala. He’s on warfarin and lithium - separate generics, monitored by a nurse who checks in every week. No fancy clinic, just a phone call and a finger prick. They don’t have fancy FDA guidelines there, but they’ve got community trust and consistent follow-up. Maybe the real problem isn’t the science - it’s that we’ve outsourced care to algorithms and profit margins. In India, if your meds change, your pharmacist calls you. Here? You find out when your hands start shaking and your INR’s through the roof.
Damario Brown
January 16, 2026so like... why dont we just make the generics match the brand better? like duh. its not that hard. i mean, i got switched to generic levothyroxine and my heart was racing for a week. then i went back to brand and boom. fine. so why cant they just make the combo pills work? its not rocket science. also why do i need a phd to understand this? i just wanna not die.
sam abas
January 17, 2026Let’s not pretend this is a regulatory failure. It’s a market failure. The pharmaceutical industry doesn’t want generics for combo NTI drugs because they can’t charge $1,200/month for them. The FDA’s ‘tightened standards’ are a smokescreen - a way to pretend they’re protecting patients while letting Big Pharma keep the gravy train rolling. And let’s be real: if a generic combo were approved tomorrow, insurers would still refuse to cover it unless the brand was $200 more expensive. The real villain isn’t the science - it’s the reimbursement structure. We’re not debating bioequivalence. We’re debating whether human life is worth more than a quarterly earnings report.
John Pope
January 18, 2026There’s a deeper truth here, buried under all the jargon: we treat drugs like math problems when they’re actually existential experiences. Warfarin isn’t a number on a lab report - it’s the silence after your spouse’s stroke. Lithium isn’t a serum level - it’s the first morning you didn’t want to die. When we reduce human survival to AUC and Cmax, we’re not regulating medicine - we’re industrializing grief. The FDA doesn’t lack standards. It lacks soul. And until we acknowledge that, no amount of precision bioequivalence modeling will fix what’s broken. You can’t quantify dignity. But you sure can charge for it.
Clay .Haeber
January 18, 2026Oh wow, the FDA finally admitted they can’t do math? Groundbreaking. Next they’ll reveal that water is wet and gravity isn’t optional. Meanwhile, patients are stuck choosing between bankruptcy and cardiac arrest. And the real joke? The same companies that profit off brand-name combos are the ones lobbying against generics. It’s like a horror movie where the monster is a spreadsheet. Congrats, America - you’ve turned pharmacology into a capitalist sudoku puzzle. And we’re all just pawns in the ‘Who Gets to Live?’ edition.
Priyanka Kumari
January 18, 2026I work in a community pharmacy in Delhi, and we’ve had patients on combo NTI meds for years. We don’t have fancy tech, but we have relationships. We call patients when their meds change. We write down their symptoms in a notebook. We sit with them. We don’t rely on algorithms - we rely on trust. The U.S. system has all the tools, but it’s forgotten the heart. Maybe the answer isn’t better math - it’s better care. Let’s invest in pharmacist-led monitoring, not just regulatory fine-tuning. Real safety isn’t in a lab report. It’s in a voice on the phone saying, ‘How are you feeling today?’
Avneet Singh
January 19, 2026Let’s be honest - this whole ‘NTI combo’ crisis is just a distraction. The real issue is that the U.S. doesn’t have universal healthcare. If everyone had access to consistent monitoring and specialist care, the ‘generic substitution’ panic would vanish. You don’t need perfect bioequivalence - you need continuity. And that’s not a pharmacology problem. It’s a political one. Stop blaming the FDA. Blame the system that lets insurance companies decide who lives and who dies. This isn’t about science. It’s about power.
Write a comment