When you pick up a generic pill at the pharmacy, you expect it to work just like the brand-name version. But how do regulators know it really does? The answer lies in something called dissolution profile comparison-a quiet but powerful tool that decides whether a generic drug is truly equivalent to the original. It’s not about ingredients alone. It’s about how fast and completely the drug releases in your body, and whether the generic matches the brand down to the last second of release.
What Is a Dissolution Profile?
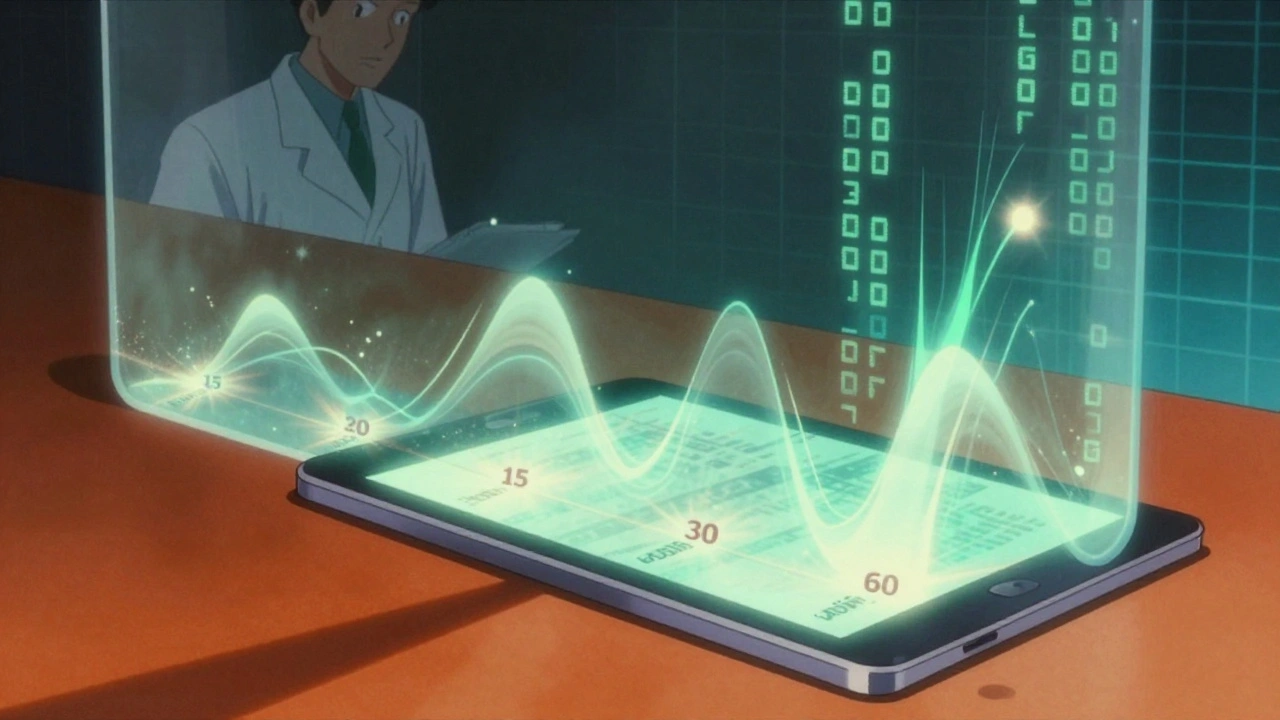
A dissolution profile is a graph that shows how much of a drug comes out of a tablet or capsule over time. Imagine dropping a pill into a liquid that mimics your stomach or intestines. Every 5, 10, 15, 30, and 60 minutes, scientists measure how much of the active ingredient has dissolved. Plot those numbers, and you get a curve-a snapshot of the drug’s behavior inside your body. This isn’t just academic. The shape of that curve determines whether the drug will be absorbed properly. If a generic dissolves too slowly, it won’t enter your bloodstream fast enough. If it dissolves too quickly, it could cause side effects. The goal? Match the brand’s curve as closely as possible.Why This Matters for Generic Drugs
Generic drug makers don’t have to repeat expensive human trials to prove their product works. Instead, they use dissolution profile comparison as a shortcut-approved by the FDA, EMA, and other global regulators. In 2022-2023, about 78% of all generic applications to the FDA relied on this method. That’s because it’s faster, cheaper, and still scientifically valid. For example, if a brand-name drug releases 80% of its active ingredient in 30 minutes, the generic must do the same under identical test conditions. That’s the baseline. But matching numbers isn’t enough. The whole curve must look alike.The f2 Similarity Factor: The Industry Standard
The most common way to compare these curves is with a number called the f2 similarity factor. It’s a statistical tool developed in 1996 and still used in over 90% of regulatory submissions today. The f2 value ranges from 0 to 100.- 100 = perfect match
- 50-100 = acceptable similarity
- Below 50 = not similar

When f2 Fails: The Hidden Problems
A 2021 study from the University of Maryland found that f2 sometimes misses real differences. In one case, two drugs had an f2 of 51-technically acceptable-but one released its drug in the first 10 minutes, while the other took 45. In vivo, that could mean one works quickly for pain relief, and the other doesn’t kick in until later. This is especially risky with drugs that have a narrow therapeutic index-like warfarin, lithium, or levothyroxine. A tiny difference in absorption can lead to overdose or underdose. That’s why the FDA’s 2023 draft guidance now recommends f2 ≥ 65 for these high-risk drugs, not just 50. Another issue? Analytical noise. A 2022 survey of 127 labs found that 73% of failed dissolution comparisons were due to equipment problems-not the drug itself. A paddle that wobbles, a vessel that’s not perfectly aligned, or a temperature off by half a degree can throw off results. That’s why labs must calibrate equipment to strict standards: shaft wobble under 1.0 mm, temperature stability within ±0.3°C, verified with NIST-traceable tools.What Happens When Profiles Don’t Match?
If the f2 score falls below 50, the generic application gets rejected. The manufacturer must go back to the drawing board. They might tweak the tablet’s binder, change the particle size, or add a surfactant to help the drug dissolve faster. One case from Teva Pharmaceuticals shows how this plays out in real life. They were developing a 25mg amlodipine tablet. Initial tests gave an f2 of 47. They adjusted the paddle alignment, increased the dissolution volume to ensure sink conditions, and retested. The new f2? 63.2. They got approval-and saved $1.2 million compared to running human bioequivalence studies. But sometimes, even a perfect f2 isn’t enough. For drugs that are poorly soluble or have complex release patterns, regulators now require more advanced tools.Beyond f2: Advanced Methods for Tough Cases
For drugs with high variability-like low-dose medications under 5mg-or those with erratic release, f2 can be misleading. That’s where alternatives come in:- Bootstrap f2: Runs the f2 calculation 1,000-10,000 times with random sampling to account for variability. More reliable than a single f2 score.
- Mahalanobis Distance Test (MDT): Looks at the entire profile as a multidimensional shape. A 2021 study showed MDT correctly identified dissimilar profiles 94% of the time-better than f2 bootstrapping’s 82%.
- AUC ratio: Compares the total area under each dissolution curve. Used alongside f2, it boosts accuracy by 23% in predicting real-world bioequivalence.
How Regulators Decide What’s Acceptable
It’s not just about numbers. Regulators look at context:- Drug class: BCS Class I drugs (highly soluble, highly permeable) are easiest to approve via dissolution. About 92% of biowaivers are for these. Class II and IV? Rarely qualify.
- Therapeutic index: High-risk drugs need tighter criteria. f2 ≥ 65 now recommended.
- Dissolution media: For BCS Class I drugs, you must test in three pH levels (1.2, 4.5, 6.8). One profile matching at pH 6.8 isn’t enough.
- Method discrimination: The test must be able to detect differences. That means intentionally stressing samples-overheating, aging, under-compressing-and proving the method picks up those changes.
What This Means for You as a Patient
You don’t need to understand the math. But you should know this: when you take a generic drug, regulators have already checked that it behaves like the brand. That’s not a guess. It’s science-rigorous, documented, and validated. The system isn’t perfect. There are rare cases where generics perform differently in real life, usually due to formulation quirks or manufacturing inconsistencies. But those are exceptions, not the rule. The vast majority of generics work just as well. And here’s the good news: the tools are getting smarter. AI is now being tested to predict in vivo performance from dissolution curves. Biorelevant media-liquids that mimic real stomach and gut conditions-are becoming standard. By 2026, these methods could become the norm.Bottom Line: Dissolution Profiles Are the Silent Gatekeepers
Dissolution profile comparison is how regulators ensure that a $5 generic pill does the same job as a $50 brand-name one. It’s not flashy. It doesn’t make headlines. But without it, the entire generic drug market would collapse. The f2 factor is the workhorse. But it’s not the whole story. Real equivalence comes from combining numbers with context, method rigor, and scientific judgment. For every generic drug you take, someone in a lab spent weeks running tests, calibrating machines, and crunching data-just to make sure you’re safe. If you ever wonder whether generics are trustworthy, remember this: they’re held to the same standard as brands-not just in ingredients, but in how they behave in your body.What is the f2 similarity factor in dissolution testing?
The f2 similarity factor is a statistical tool used to measure how similar two dissolution profiles are. It compares the percentage of drug released over time between a generic and brand-name product. An f2 value between 50 and 100 means the profiles are considered similar, with 100 being identical. It’s the most widely accepted method for regulatory approval of generic drugs.
Why is dissolution testing used instead of human bioequivalence studies for generics?
Dissolution testing is faster, cheaper, and avoids exposing volunteers to unnecessary risk. If two drug products dissolve in the same way under controlled lab conditions, regulators can reasonably assume they’ll behave the same in the body. This approach reduces development costs by up to 60% and cuts approval time by 12-18 months compared to full human trials.
Can a generic drug pass dissolution testing but still not work the same in patients?
It’s rare, but possible. Dissolution testing measures how the drug releases, not how it’s absorbed or metabolized. If a drug has complex absorption patterns, or if the patient has gut conditions that affect absorption, real-world performance may vary. However, regulatory agencies require discriminatory methods and multiple pH tests to minimize this risk. Most failures are due to lab error, not drug design.
What drugs are most likely to have issues with dissolution profile matching?
Drugs with low solubility (BCS Class II and IV), very low doses (under 5mg), or narrow therapeutic indexes (like warfarin, digoxin, or levothyroxine) are hardest to match. These require more rigorous testing, including multiple dissolution media, bootstrap f2, or Mahalanobis Distance Test. BCS Class I drugs (high solubility and permeability) are easiest to approve via dissolution.
Are there new methods replacing f2 in dissolution testing?
f2 is still the standard, but new methods are gaining ground. Bootstrap f2, Mahalanobis Distance Test, and AUC ratio are increasingly used for high-risk drugs. The FDA and EMA are also pushing for biorelevant dissolution media-liquids that mimic stomach and intestinal fluids. AI models are being piloted to predict in vivo performance from dissolution curves. These won’t replace f2 yet, but they’re becoming essential tools for complex cases.








Comments
मनोज कुमार
December 3, 2025Dissolution profiles f2 factor 50-100 acceptable but who checks the lab equipment calibration most times its just sloppy technique not the drug itself
Joel Deang
December 5, 2025so like if the generic dissolves too fast u get a rush right? like a caffeine hit but for pills?? 😅 i always thought generics were just cheaper copies but this is wild
Arun kumar
December 6, 2025its funny how we trust pills so much without knowing how they work inside us. the science behind this is quiet but it holds up the whole system. someone in a lab spent weeks just to make sure your headache pill works the same as the expensive one. we dont see it but its there
ATUL BHARDWAJ
December 8, 2025f2 is just a number real equivalence needs more
Steve World Shopping
December 10, 202590% of generic approvals rely on f2? that's a regulatory loophole disguised as science. if you cant prove bioequivalence in humans then you're gambling with lives. this is how pharma cuts corners
Alicia Marks
December 10, 2025So cool to see how much science goes into something so simple! You're right-generics are safe and this is why. 🙌
Paul Keller
December 12, 2025While the f2 similarity factor is widely adopted, its statistical limitations are often ignored by regulatory bodies. The assumption that a single metric can encapsulate the entire pharmacokinetic behavior of a drug is fundamentally flawed. Dissolution profiles are multidimensional phenomena, and reducing them to a single scalar value-especially one that is sensitive to minor analytical deviations-creates a false sense of security. The FDA’s own 2023 draft guidance acknowledging higher thresholds for narrow-therapeutic-index drugs is a step in the right direction, but it remains reactive rather than proactive. A paradigm shift toward multivariate analysis and biorelevant media is not just advisable-it is imperative for patient safety.
Shannara Jenkins
December 13, 2025This is actually really reassuring! I used to worry about generics but now I see how much care goes into making sure they’re just as good. Thanks for breaking it down so clearly 💛
Elizabeth Grace
December 14, 2025I just took my levothyroxine this morning and now I’m paranoid. What if my generic didn’t match the curve? 😭
Steve Enck
December 14, 2025It is not merely a matter of statistical compliance; it is an epistemological failure of regulatory science. The f2 factor, as a deterministic metric, cannot account for stochastic biological variability. Its widespread use represents a systemic capitulation to cost-efficiency over epistemic rigor. One must question whether the regulatory apparatus has become a tool of pharmaceutical commodification rather than a guardian of public health. The data is not the reality; the curve is not the body.
Jay Everett
December 16, 2025Man, this whole thing is like a secret superhero origin story for your pills 💥 The lab techs with their calibrated paddles and NIST-traceable thermometers? They’re the real MVPs. And now with AI and biorelevant media coming in? We’re gonna have pills that predict how *you* absorb them. Wild. 🤯 Keep pushing the science-this is how we make medicine smarter, not just cheaper.
Write a comment