
Hashimoto’s thyroiditis is the most common cause of hypothyroidism in the United States, affecting about 4% of adults - that’s nearly 10 million people. It’s not just a slow thyroid. It’s your immune system turning against your own thyroid gland, slowly destroying its ability to make hormones. For many, symptoms creep in quietly: fatigue that won’t lift, weight gain despite eating less, brain fog, cold hands, and a voice that feels hoarse. By the time they see a doctor, the damage is already done. But here’s the good news: with the right monitoring and treatment, most people can live symptom-free. The key? Understanding TSH - and why it’s the single most important number in managing this condition.
What Exactly Is Hashimoto’s Thyroiditis?
Hashimoto’s isn’t just hypothyroidism. It’s autoimmune hypothyroidism. That means your body’s defense system - meant to fight viruses and bacteria - starts attacking your thyroid. It produces antibodies, especially thyroid peroxidase antibodies (TPOAb), that damage thyroid cells. Over time, the gland can’t keep up with hormone production. The result? Low thyroid hormone levels, which slow down your metabolism, energy, heart rate, and even your mood.
This isn’t rare. In iodine-sufficient areas like the U.S., Hashimoto’s causes about 90% of all hypothyroidism cases. Women are five to ten times more likely to develop it than men. It often shows up between ages 30 and 50, but it can strike at any age. Family history plays a role. So do other autoimmune conditions like type 1 diabetes, celiac disease, or rheumatoid arthritis.
Unlike some thyroid problems, Hashimoto’s doesn’t go away. Once your immune system starts attacking, it doesn’t stop. But the good news? You don’t need to fix the immune system to feel better. You just need to replace what your thyroid can’t make anymore.
Why TSH Is the Gold Standard for Monitoring
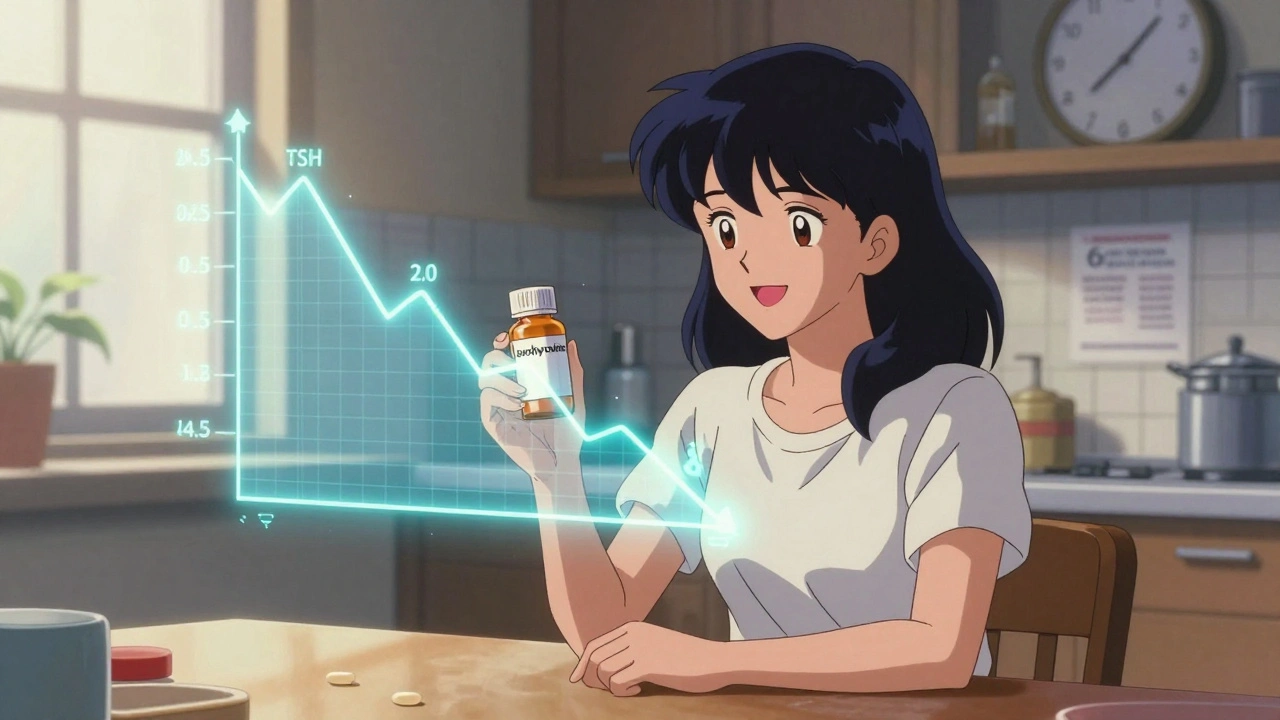
When doctors check your thyroid, they don’t just look at T4 or T3. They start with TSH - thyroid-stimulating hormone. Why? Because TSH tells you what your brain thinks your thyroid is doing.
Your pituitary gland, right behind your brain, constantly checks how much thyroid hormone is in your blood. If levels drop, it pumps out more TSH to tell the thyroid to work harder. If levels rise too high, it cuts back. So when your thyroid is failing, TSH shoots up - often long before T4 drops into the abnormal range.
That’s why TSH is the first test. If your TSH is above 4.5 mIU/L, doctors will check your free T4 and TPO antibodies. A high TSH with low T4 means you have overt hypothyroidism. A high TSH with normal T4? That’s subclinical hypothyroidism - still worth treating if you have symptoms or positive antibodies.
And here’s the critical part: once you’re on levothyroxine, TSH is the only test you need for monitoring. The Cleveland Clinic, the American Thyroid Association, and the American Association of Clinical Endocrinologists all agree. You don’t need to check T4 or T3 every few months. TSH alone tells you if your dose is right.
How Levothyroxine Works - And Why Timing Matters
Levothyroxine (LT4) is synthetic T4. It’s identical to the hormone your thyroid used to make. Your body converts it into T3, the active form, as needed. The goal isn’t to make your TSH normal - it’s to make it stable and within your personal target range.
Dosing starts around 1.4 to 1.8 mcg per kilogram of body weight. For a 70 kg adult, that’s about 100 mcg/day. But many doctors start lower - 25 to 50 mcg - especially in older adults or those with heart conditions. Why? Because too much too fast can cause palpitations or even trigger a heart rhythm problem.
It takes time for your body to adjust. Levothyroxine has a half-life of about 7 days. That means it takes 4 to 6 weeks for your TSH to fully respond to a dose change. That’s why doctors won’t adjust your dose every month. If you change your dose on January 1st, you won’t get tested until late February or early March. Waiting 6 to 8 weeks isn’t a delay - it’s science.
Many patients get frustrated. They feel worse for weeks after a dose increase and think the medicine isn’t working. But it’s not the medicine. It’s your body catching up. Patience matters.
What Your TSH Target Should Be
Not everyone’s ideal TSH is the same. The standard lab range is 0.4 to 4.0 mIU/L. But that’s a population average. Your personal target might be different.
For most adults under 65, aiming for 0.5 to 2.5 mIU/L is common. That’s the sweet spot where most people feel their best. Some studies, including a 2023 JAMA Internal Medicine study of over 12,000 people, found that those with a specific gene variant (DIO2) felt significantly better when TSH was kept in the lower half of normal - between 0.4 and 2.0.
For older adults - especially those over 65 - a slightly higher TSH (up to 6.0 mIU/L) is often acceptable. Why? Because pushing TSH too low in older people can increase bone loss and heart risks. The American Academy of Family Physicians supports this more relaxed approach for seniors.
Pregnancy changes everything. If you’re trying to conceive or already pregnant, your target drops sharply. In the first trimester, TSH should be under 2.5 mIU/L. By the third trimester, it can go up to 3.0. Why? Because your baby depends on your thyroid hormones in the first 12 weeks - before its own thyroid even starts working. If your TSH is too high during pregnancy, your baby’s brain development can be affected. That’s why pregnant women with Hashimoto’s get tested every 4 weeks until week 20.
When and How Often to Test
Testing frequency follows a clear pattern:
- After starting levothyroxine: retest TSH in 6 to 8 weeks
- After any dose change: wait 6 to 8 weeks before retesting
- Once stable: test once a year
Some patients need more frequent checks. If you’ve gained or lost more than 10% of your body weight, started or stopped estrogen pills, began taking iron or proton pump inhibitors (like omeprazole), or started a new medication, your dose may need adjustment. These can interfere with how well your body absorbs levothyroxine.
And yes - if you’re feeling off, don’t wait. Tell your doctor. Fatigue, weight gain, depression, or cold intolerance could mean your dose is too low. Anxiety, heart racing, trouble sleeping, or unexplained weight loss? That could mean you’re over-replaced. Symptoms matter - even if your TSH is technically in range.
What You Shouldn’t Waste Time On
Many patients obsess over their TPO antibody levels. They get tested every few months, hoping the numbers will drop. But they won’t. And it doesn’t matter.
The American Thyroid Association is clear: “Repeating and monitoring your thyroid antibody levels is not needed.” Antibodies tell you the cause - not the severity or treatment response. You can have sky-high antibodies and feel great on the right dose. Or low antibodies and still feel terrible if your TSH is off.
Same goes for T3. Routine T3 testing isn’t recommended. Your body converts T4 to T3 as needed. Adding synthetic T3 (like Cytomel) is only considered in rare cases where someone still has symptoms despite normal TSH and T4 - and even then, evidence is weak. The Cochrane Review found no consistent benefit from adding T3 to standard treatment.
Real-Life Challenges and What to Do About Them
People with Hashimoto’s often feel dismissed. “Your labs are normal, so you’re fine.” But labs don’t tell the whole story. If you’re still tired, gaining weight, or struggling with brain fog - even with a TSH of 3.0 - talk to your doctor about lowering your target to 1.5 or 2.0. Some patients do better at the lower end.
Another big issue: absorption. Levothyroxine works best on an empty stomach. Take it 30 to 60 minutes before breakfast. Don’t take it with coffee, calcium, iron, or soy - they block absorption. If you take a multivitamin with iron, take it at night. If you’re on acid blockers, your dose might need adjusting.
And don’t switch brands unless you have to. Generic levothyroxine is fine for most people. But because of FDA regulations since 2018, potency varies slightly between manufacturers. If you switch and start feeling different, tell your doctor. You may need a dose tweak.
What’s Next for Hashimoto’s Management?
Research is moving fast. In 2021, the FDA approved the first home TSH test - ThyroChek. It’s not yet recommended for routine use, but it’s a sign of things to come. In the future, people with stable Hashimoto’s might test at home every few months instead of visiting a lab.
Personalized medicine is also gaining ground. Genetic testing for DIO2 variants could soon help doctors pick your ideal TSH target before you even start treatment. And while combination T4/T3 therapy remains controversial, ongoing trials are exploring whether certain patients - like those with persistent fatigue - benefit from a tailored approach.
For now, though, the path is clear: take your levothyroxine daily, get your TSH checked at the right times, and don’t let antibody numbers drive your treatment. You’re not broken. Your thyroid just needs a little help - and with that, you can feel like yourself again.
Can Hashimoto’s thyroiditis be cured?
No, Hashimoto’s thyroiditis cannot be cured. It’s a lifelong autoimmune condition where the immune system attacks the thyroid. But it can be effectively managed with daily levothyroxine medication. Once your TSH is stabilized, most people experience no symptoms and live normal, healthy lives.
Why is my TSH normal but I still feel tired?
Even with a normal TSH, you might still feel fatigued if your target range isn’t personalized. Many people feel best when their TSH is between 0.5 and 2.0, not just within the lab’s 0.4-4.0 range. Other factors like iron deficiency, vitamin D levels, sleep quality, or stress can also contribute. Talk to your doctor about adjusting your target and checking for other causes.
Do I need to avoid gluten with Hashimoto’s?
There’s no strong evidence that gluten causes Hashimoto’s or that avoiding it will improve thyroid function - unless you have celiac disease. Some people report feeling better on a gluten-free diet, possibly due to reduced inflammation. But it’s not a required treatment. If you want to try it, do so under medical supervision and don’t replace proven treatment with diet alone.
Can I stop taking levothyroxine if I feel better?
No. Levothyroxine replaces what your thyroid can no longer make. Stopping it - even if you feel fine - will cause your TSH to rise again and symptoms to return. It’s not a cure, it’s a replacement. Think of it like insulin for diabetes: you take it because your body doesn’t make enough, not because you’re temporarily sick.
How long does it take to feel better after starting levothyroxine?
Most people notice small improvements in energy and mood within 2 to 3 weeks. But full symptom relief often takes 6 to 8 weeks - the time it takes for your body to fully adjust to the new hormone level and for your TSH to stabilize. Don’t rush dose changes. Wait at least 6 weeks between adjustments.
Should I get my thyroid antibodies tested regularly?
No. The American Thyroid Association says antibody testing is not needed for ongoing management. Antibody levels don’t predict how you’ll feel or how well your treatment is working. They only confirm the autoimmune cause at diagnosis. Focusing on TSH and symptoms is far more useful for daily care.
Can Hashimoto’s affect my mental health?
Yes. Low thyroid hormone levels are strongly linked to depression, anxiety, brain fog, and memory issues. Many people with untreated Hashimoto’s are misdiagnosed with depression. Once treated properly, these symptoms often improve significantly. If mood problems persist despite normal TSH, other factors like sleep, stress, or neurotransmitter imbalances should be evaluated.






Comments
Carolyn Woodard
December 1, 2025It’s fascinating how TSH functions as a feedback loop sentinel-essentially the hypothalamic-pituitary-thyroid axis acting as a biological thermostat. What’s often missed is that TSH isn’t just a marker; it’s a dynamic signal reflecting tissue-level deiodinase activity, particularly DIO2 expression in the brain and muscle. The 2023 JAMA study you cited aligns with emerging epigenetic data showing that individuals with certain DIO2 polymorphisms may require lower TSH targets not because their thyroid is failing, but because their neural conversion efficiency is genetically optimized for a narrower range. We’re moving beyond population averages into personalized endocrinology.
Allan maniero
December 3, 2025Look, I’ve been on levothyroxine for twelve years now, and I’ve seen the whole circus-from doctors who treat TSH like a goddamn holy number to those who ignore symptoms entirely because ‘it’s in range.’ The truth? Your body doesn’t care about lab ranges. It cares about how you feel. I used to be told my TSH was fine at 3.8, but I was dragging myself through the day like a zombie. When I pushed for a target of 1.7, everything changed-sleep improved, brain fog lifted, even my cold hands warmed up. Don’t let a computer-generated reference interval dictate your quality of life. You know your body better than any algorithm.
william tao
December 4, 2025Let me be perfectly clear: the notion that TSH alone is sufficient for monitoring is a dangerous oversimplification propagated by pharmaceutical-aligned guidelines. The American Thyroid Association receives funding from major levothyroxine manufacturers. The Cochrane Review you cite? It excluded studies using natural desiccated thyroid. Why? Because it doesn’t fit the narrative. If you're still symptomatic with a 'normal' TSH, you're not imagining it-you're being gaslit by a system that prioritizes cost-efficiency over clinical nuance.
Sandi Allen
December 5, 2025STOP. LISTEN. THEY’RE HIDING THE TRUTH! TSH ISN’T THE REAL PROBLEM-IT’S THE GLUTEN! THE FLUORIDE! THE 5G! THEY’RE ALL WORKING TOGETHER TO KEEP YOU SICK SO YOU’LL KEEP BUYING LEVOTHYROXINE! I DID A 30-DAY GLUTEN-FREE CHALLENGE AND MY TPO ANTIBODIES DROPPED 40%! THEY DON’T WANT YOU TO KNOW THIS BECAUSE IT’S NOT PROFITABLE! I’VE BEEN RESEARCHING THIS FOR 7 YEARS AND NOBODY LISTENS! I’M JUST A NORMAL PERSON WHO WANTS TO BE HEALTHY!!
Eddy Kimani
December 6, 2025This is one of the clearest breakdowns of Hashimoto’s management I’ve seen. The emphasis on TSH as a stable target-not just a ‘normal’ number-is crucial. I’ve had patients who felt awful at TSH 2.8 and great at 1.9, despite both being ‘in range.’ The key insight here is that optimal isn’t the same as normal. And the point about absorption? So many miss that. Coffee, calcium, iron-all silent saboteurs. I always tell my patients: take it like a sacrament. Empty stomach. No interference. Wait 30 minutes. It’s not optional-it’s pharmacokinetics.
Chelsea Moore
December 7, 2025I CAN’T BELIEVE PEOPLE ARE STILL BUYING INTO THIS! I’M A 34-YEAR-OLD WOMAN WHO’S BEEN ON THYROID MEDS FOR 8 YEARS, AND MY DOCTOR STILL TELLS ME ‘IT’S JUST A TSH THING’-WHEN I’M SO TIRED I CAN’T GET OUT OF BED! I’VE TRIED EVERYTHING-SELENIUM, VITAMIN D, GLUTEN-FREE, KETO, EVEN CRYO THERAPY! WHY WON’T ANYONE LISTEN?! I JUST WANT TO FEEL LIKE MYSELF AGAIN AND NOBODY GETS IT!!
John Biesecker
December 8, 2025man i’ve been here too 😔 same story-tsh at 3.5, still exhausted, cold all the time, brain like wet cardboard. then i found a doc who actually listened and lowered my target to 1.8. changed my life. i still take it on empty stomach, no coffee for an hour, and i swear by taking it before bed now (yes, that works for some of us). also-dont stress about antibodies. they’re just the reason you’re here, not the problem you’re solving. you’re not broken. your thyroid just needs a nudge. 🙌🫶
Genesis Rubi
December 10, 2025Why are we even letting these American doctors decide what’s best? In Europe, they use natural thyroid extracts. In Japan, they test free T3 and T4 routinely. This whole TSH obsession is pure American medical laziness. We’re being sold a cheap synthetic hormone and told to shut up and take it. Meanwhile, real medicine is happening elsewhere. Why are we accepting this? It’s embarrassing.
Write a comment